

We have been discussing the use of CBCT in the practice of endodontics. There have been questions about whether CBCT is really necessary, or just another cool image. That particular question was one of the biggest we had in our decision to move to CBCT. We also ask that question to ourselves when we recommend a CBCT scan to our patients. However, much like a microscope, until you look through the scope, you often don’t know what you are missing. I have found that quite regularly, I will find things that I could not have seen otherwise and it has changed the treatment that I have recommended.
Here’s an example of a routine CBCT scan that I did prior to endodontic surgery. This scan gave me added information, that then changed the treatment plan and give us better prognosis.
This patient presented for evaluation. The teeth are asymptomatic, but a lesion seen by his general dentist. The lesion is obviously on the MB root of #3, with ledged MB canal. The crown margins looked good and since the MB canal is ledged, we were planning to treat this tooth with an apicoectomy. I recommended a routine, pre-surgical CBCT to evaluate the root anatomy, sinus proximity and buccal bone contours.

This slice through the MB root shows that there is a missed MB#2 canal.
A slice through the palatal root shows a periapical lesion on the palate not visible in the original, pre-op radiograph. This now changes our treatment recommendation. An apicoectomy will resolve the MB issues, but fail to resolve the palatal lesion. This could cause continued problems and lead to the assumption of a failed endodontic surgery, when the palatal root could be the problem.

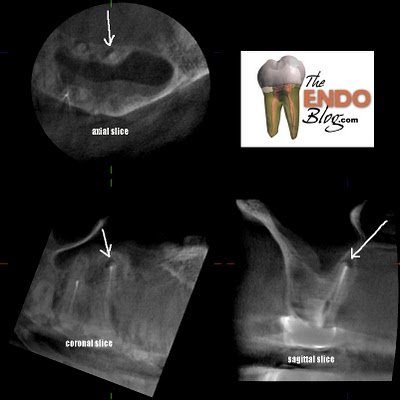
An additional slice through the palatal roots shows that #2 also has a significant periapical lesion requiring treatment.

A sagittal view of #2 again shows the extent of the lesion.
While the lesion on the palate of #2 is visible in the original radiograph, there is no doubt about it’s presence with the sagittal view above.
In this case the additional information about the palatal lesion on #3 changed the treatment recommendation and will thereby improve the prognosis. Lack of CBCT scan in this case would have led to wrong treatment recommendation.
That being said, I know there are those who will say…”alway retreat first” and you don’t need a CBCT scan to make that decision.
CBCT provides improved imaging of the the teeth and periapex. I welcome the added information into the diagnostic and treatment part of my practice. For more information about the application of CBCT into endodontics, the upcoming Inner Space Seminar is right around the corner.
